
Randomized controlled trials sit at the top of the evidence hierarchy in scientific research, and for good reason. When researchers want to know whether a treatment, drug, or intervention actually causes an outcome, rather than merely coinciding with it, an RCT offers the most reliable way to find out. By randomly assigning participants to either a treatment group or a control group, researchers can strip away the influence of confounding variables and bias, isolating the true effect of whatever is being tested.
This design underpins decisions in medicine, public health, economics, and social science, from approving new drugs to evaluating education programs. Understanding how RCTs work, including concepts like randomization, control groups, and blinding, helps you interpret the strength of a study’s claims.
What Is a Randomized Controlled Trial?
A randomized controlled trial (RCT) is a study design in which participants are randomly assigned to one of two or more groups to test the effect of a treatment, intervention, or exposure. One group, the treatment group, receives the intervention being studied, while another, the control group, receives a placebo, standard treatment, or no intervention at all. Because assignment is random, each participant has an equal chance of ending up in either group, regardless of their personal characteristics, health status, or preferences.
This random allocation is what sets RCTs apart from observational studies. It ensures that, on average, the groups being compared are similar in every way except for the intervention itself, so any difference observed in outcomes can be attributed to the treatment rather than to some other underlying factor.
RCTs are widely regarded as the gold standard for establishing cause-and-effect relationships, particularly in clinical medicine, but also in fields such as economics, psychology, and public policy.
Key Features of a Randomized Controlled Trial
Randomization
Participants are assigned to groups using a chance-based process, such as a random number generator or computer algorithm, rather than by choice or convenience. This prevents researchers or participants from influencing who ends up in which group, guarding against selection bias.
Control Group
Every RCT includes at least one control group that does not receive the experimental treatment. This group serves as a benchmark, allowing researchers to compare outcomes and determine whether the treatment produced an effect beyond what would have happened anyway.
Blinding
Many trials use blinding to prevent expectations from influencing outcomes. In a single-blind trial, participants don’t know which group they’re in. In a double-blind trial, neither participants nor researchers know, which helps prevent bias in how symptoms are reported or interpreted.
Predefined Protocol
RCTs follow a detailed plan established before the trial begins, specifying the hypothesis, sample size, procedures, and outcome measures. This reduces the risk of researchers adjusting methods partway through in ways that could skew results.
Sample Size and Power
Trials are designed with a sample size large enough to detect a meaningful effect if one exists, based on a statistical power calculation. An underpowered trial risks missing a real effect, while an unnecessarily large one wastes resources.
How a Randomized Controlled Trial Works
While the specifics vary by field and study, most RCTs follow a similar sequence of steps from design through analysis.
1. Formulating the Research Question and Hypothesis
Researchers start by defining a clear, testable hypothesis, typically stated as a null hypothesis () that the intervention has no effect, against an alternative hypothesis () that it does.
2. Determining Eligibility Criteria
Inclusion and exclusion criteria are set to define exactly who can participate, ensuring the sample matches the population the results are meant to generalize to.
3. Calculating Sample Size
Using a power analysis, researchers estimate how many participants are needed to detect a meaningful effect, based on the expected effect size, desired statistical power (commonly 0.80), and significance level (commonly ).
4. Randomly Assigning Participants
Eligible participants are allocated to the treatment or control group using a random process. Common methods include simple randomization, block randomization, and stratified randomization, the latter used to balance known variables like age or sex across groups.
5. Implementing Blinding
Where feasible, participants, clinicians, and sometimes data analysts are kept unaware of group assignment to reduce bias in how outcomes are reported or measured.
6. Delivering the Intervention
The treatment group receives the intervention being tested, while the control group receives a placebo, an existing standard treatment, or no intervention, depending on the study design.
7. Monitoring and Data Collection
Researchers track participants over the course of the trial, recording outcomes, side effects, and any dropouts according to the predefined protocol.
8. Analyzing the Results
Once data collection ends, researchers compare outcomes between groups using statistical tests appropriate to the data, calculating a p-value and confidence interval to determine whether observed differences are statistically significant.
9. Reporting Findings
Results are published, typically following standardized reporting guidelines such as CONSORT, which promote transparency about methodology, participant flow, and any limitations encountered.
Types of Randomized Controlled Trials
Parallel-Group Trials
The most common design, in which each participant is assigned to one group, either treatment or control, for the entire duration of the study. Outcomes between the groups are compared at the end of the trial.
Crossover Trials
Participants receive both the treatment and the control (or multiple treatments) in a sequence, separated by a washout period to eliminate carryover effects. Each participant effectively serves as their own control, which can reduce the number of participants needed, though this design isn’t suitable for treatments with lasting or permanent effects.
Cluster Randomized Trials
Instead of randomizing individual participants, entire groups, such as schools, clinics, or communities, are randomly assigned to treatment or control conditions. This design is useful when an intervention naturally applies at a group level, such as a public health campaign or a policy change.
Factorial Trials
These trials test two or more interventions simultaneously by assigning participants to combinations of treatments, such as Treatment A alone, Treatment B alone, both, or neither. This design allows researchers to study interactions between treatments efficiently within a single trial.
Adaptive Trials
The trial design allows for planned modifications, such as adjusting sample size, dropping ineffective treatment arms, or reallocating participants, based on interim data analysis. This flexibility can speed up trials and reduce exposure to ineffective treatments, though it requires careful statistical planning to avoid introducing bias.
Non-Inferiority and Equivalence Trials
Rather than testing whether a new treatment is better than a control, these trials assess whether it is no worse (non-inferiority) or clinically equivalent (equivalence) to an existing standard treatment, often used when a new option offers other advantages like lower cost or fewer side effects.
Examples of Randomized Controlled Trials
Randomized controlled trials appear across many disciplines, not just medicine. The following examples illustrate how the design is applied in practice.
Vaccine Efficacy Trials
A common application in medicine involves testing a new vaccine against a placebo. Participants are randomly assigned to receive either the vaccine or a saline injection, and researchers track infection rates in both groups over a defined period. Because assignment is random and often double-blind, any difference in infection rates can be attributed to the vaccine itself rather than differences in participants’ behavior or immune systems.
Drug Trials for Chronic Conditions
In testing a new medication for a condition like high blood pressure, participants are randomized to receive either the new drug or a standard existing treatment. Outcomes such as changes in blood pressure readings are compared between groups after a set treatment period, often using a crossover design if the condition and treatment allow for it.
Educational Intervention Studies
Researchers might randomly assign classrooms or schools (a cluster randomized design) to either adopt a new teaching method or continue with the standard curriculum. Student performance on standardized assessments is then compared between the two conditions to determine whether the new method improves learning outcomes.
Behavioral and Public Health Trials
A public health study might randomize participants to receive text-message reminders promoting physical activity versus no reminders at all, measuring changes in self-reported exercise levels or step counts over several weeks.
Economic and Policy Trials
In development economics, researchers have used RCTs to test interventions such as providing cash transfers to some randomly selected households while withholding them from others, then comparing outcomes like income, spending habits, or school enrollment between groups.
Website and Product Testing (A/B Testing)
Though rarely labeled as an RCT in casual use, A/B testing follows the same logic: users are randomly shown different versions of a webpage or app feature, and engagement metrics are compared to determine which version performs better.
Real-World Example: The RECOVERY Trial (Dexamethasone for COVID-19)
One of the most influential randomized controlled trials in recent history is the RECOVERY Trial, a large, multi-armed, adaptive platform trial launched in the UK in March 2020 to test potential treatments for hospitalized COVID-19 patients.
For its dexamethasone arm, researchers randomized 6,425 patients in a 1:2 ratio to either 6 mg of dexamethasone daily for 10 days or usual care. Because assignment was random, the two groups were comparable in age, illness severity, and other characteristics at the outset, meaning any difference in outcomes could be attributed to the drug itself. clinicaltrials
The results were striking: 28-day mortality was significantly lower in the dexamethasone group at 22.9%, compared with 25.7% in the control group. Patients on dexamethasone also had shorter hospital stays and a greater likelihood of being discharged within 28 days. Notably, dexamethasone offered no benefit to patients who did not require supplemental oxygen, illustrating how RCTs can reveal not just whether a treatment works, but for whom. 2 Minute Medicine + 2
These findings, published in the New England Journal of Medicine, rapidly changed clinical practice worldwide and remain a textbook example of how a well-designed RCT can generate reliable, actionable evidence in the middle of a global health crisis. Full trial documentation and results are available on the RECOVERY Trial website.
How to Know If a Study Is an RCT
Not every study that mentions “randomized” or “controlled” is a true RCT, so it helps to know exactly what to look for when reading a paper or its abstract.
Look for Explicit Random Assignment
The clearest sign is a direct statement that participants were randomly assigned to groups, often naming the method used, such as computer-generated randomization, random number tables, or block randomization. If participants were assigned based on convenience, preference, or an existing characteristic, it isn’t a true RCT.
Check for a Control or Comparison Group
A genuine RCT compares the treatment group against a control group receiving a placebo, standard care, or no intervention. A study with only one group and no comparison arm is not an RCT, regardless of how rigorous its measurements are.
Look at the Methods Section, Not Just the Title
Titles and abstracts sometimes use “randomized” loosely or inaccurately. The methods section should describe the randomization procedure in detail, including how allocation was concealed from those enrolling participants, which helps confirm the randomization was genuine and not manipulated.
Check for a Trial Registration Number
Most legitimate RCTs are registered in advance on a public database, such as ClinicalTrials.gov, and the paper will typically cite a registration number (for example, an NCT number). Pre-registration reduces the risk of selective reporting and supports the credibility of the trial.
Look for a CONSORT Flow Diagram
Many published RCTs include a flow diagram, following CONSORT guidelines, showing how many participants were assessed, randomized, allocated to each group, and analyzed. The presence of this diagram is a strong indicator of a properly conducted RCT.
Identify the Type of Blinding Used, If Any
The methods section should specify whether the trial was open-label, single-blind, or double-blind. While blinding isn’t required for a study to count as an RCT, its absence or presence should be clearly stated rather than left ambiguous.
Watch for Red Flags
Be cautious of studies labeled as “randomized” that lack a clear allocation method, have very small or uneven group sizes without explanation, or don’t specify how outcomes were measured and by whom, as these can indicate a poorly designed or misrepresented trial.
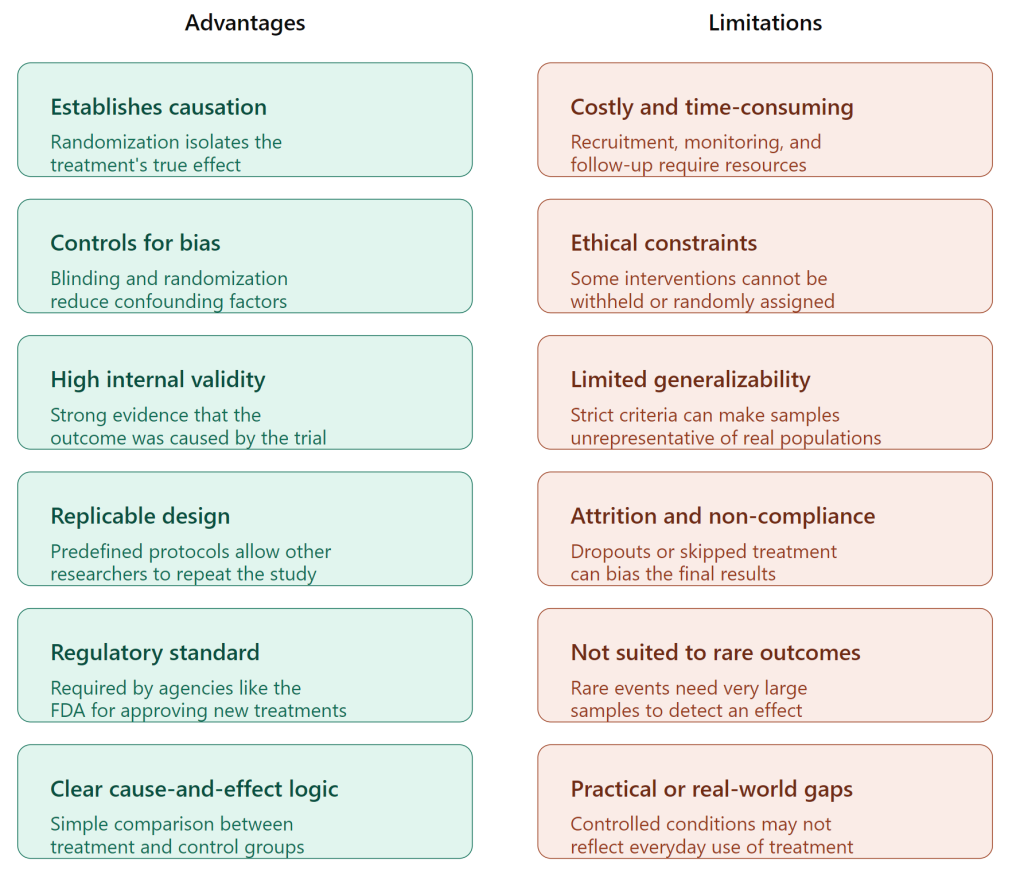
Advantages and Limitations of Randomized Controlled Trials
RCT vs Other Research Methods
RCTs vs Observational Studies
Observational studies simply record what happens without assigning any intervention, meaning researchers observe existing groups rather than creating them through randomization. This makes them easier and cheaper to conduct, but far more vulnerable to confounding variables, since the groups being compared may differ in ways beyond the exposure of interest. RCTs address this by randomly assigning participants, which balances both known and unknown confounders across groups.
RCTs vs Cohort Studies
A cohort study follows a group of people over time, comparing outcomes between those who were exposed to a factor, such as smoking, and those who weren’t. Because exposure isn’t randomly assigned, differences between groups may reflect underlying lifestyle or health factors rather than the exposure itself. Cohort studies are useful when randomization is unethical or impractical, such as studying the long-term effects of smoking, but they generally offer weaker evidence of causation than an RCT.
RCTs vs Case-Control Studies
Case-control studies work backward, starting with people who already have an outcome, such as a disease, and comparing them to people who don’t, looking back at past exposures. This design is efficient for studying rare conditions but is prone to recall bias and cannot establish causation with the same confidence as an RCT, since exposure history is reconstructed rather than controlled.
RCTs vs Quasi-Experiments
Quasi-experiments resemble RCTs in that they test an intervention’s effect, but they lack random assignment, instead relying on naturally occurring groups or a specific rule to divide participants, such as a policy change that comes into effect on a certain date. They’re often used when randomization is impossible for ethical, legal, or logistical reasons, but the absence of randomization leaves more room for selection bias to explain the observed results.
RCTs vs Cross-Sectional Studies
A cross-sectional study captures a snapshot of a population at a single point in time, measuring the presence of an exposure and an outcome simultaneously. This design can reveal associations and is useful for estimating prevalence, but it cannot establish the order of events, so it’s unable to determine whether the exposure caused the outcome or vice versa.
Importance of RCTs in Evidence-Based Practice
Minimizing Bias in Decision-Making
Because randomization balances both known and unknown confounding variables across groups, RCTs provide a level of confidence in cause-and-effect relationships that other study designs struggle to match. This matters enormously when the findings will shape decisions affecting large numbers of people, such as approving a new drug or funding a national program.
Informing Clinical Guidelines
Medical bodies and regulatory agencies rely heavily on RCT data when developing treatment guidelines. A single well-designed RCT, or more often a meta-analysis combining several, can shift standard practice, as seen when the RECOVERY Trial’s dexamethasone findings changed COVID-19 treatment protocols worldwide within weeks of publication.
Supporting Systematic Reviews and Meta-Analyses
RCTs form the backbone of systematic reviews, which pool results from multiple trials to produce more precise and generalizable estimates of an effect. Because RCTs share a common logic of randomization and control, their results are easier to compare and combine than those from observational studies.
Guiding Policy and Program Evaluation
Beyond medicine, RCTs increasingly inform decisions in education, economics, and social policy. Governments and organizations use them to test whether an intervention, such as a cash transfer program or a classroom teaching method, produces the intended effect before scaling it up.
Building Public Trust
Because RCTs are transparent about their methodology and often preregistered, they help build confidence that reported findings reflect a treatment’s real effect rather than bias, chance, or selective reporting. This transparency is part of why regulatory bodies such as the FDA require RCT evidence before approving new drugs.
Limitations to Keep in Mind
Despite their strength, RCTs are not a substitute for judgment. Findings from a trial conducted in one population, setting, or time period don’t always generalize perfectly to another, which is why evidence-based practice also draws on cohort studies, clinical experience, and context-specific knowledge alongside RCT data.
Common Terms Related to RCTs
Randomization
The process of assigning participants to treatment or control groups using chance, such as a random number generator, to eliminate selection bias.
Control Group
The group in a trial that does not receive the experimental intervention, serving as a baseline for comparison.
Placebo
An inactive substance or sham treatment given to the control group so it resembles the real intervention, helping isolate the treatment’s true effect from psychological or behavioral responses.
Blinding
A technique used to prevent participants (single-blind) or both participants and researchers (double-blind) from knowing group assignment, reducing the risk of bias in reporting or interpreting outcomes.
Intention-to-Treat (ITT) Analysis
An analysis approach that includes all randomized participants in their originally assigned group, regardless of whether they completed or adhered to the treatment, preserving the benefits of randomization.
Per-Protocol Analysis
An analysis that includes only participants who followed the trial protocol as intended, which can offer insight into the treatment’s effect under ideal conditions but risks introducing bias.
Attrition
The loss of participants from a trial over time due to dropout, withdrawal, or loss of contact, which can affect the validity of results if it occurs unevenly between groups.
Effect Size
A quantitative measure of the magnitude of difference between groups, such as a mean difference or odds ratio, independent of sample size.
Confidence Interval (CI)
A range of values, typically set at 95%, within which the true effect size is likely to fall, providing a sense of the precision of an estimate.
p-valueA statistical measure indicating the probability of observing results as extreme as those found, assuming the null hypothesis is true; a p-value below a predetermined threshold (commonly α=0.05) is often considered statistically significant.
Statistical Power
The probability that a trial will detect a true effect if one exists, commonly set at 0.80, influenced by sample size, effect size, and significance level.
Stratified Randomization
A method of randomization that ensures balance across known variables, such as age or disease severity, by randomizing within predefined subgroups before combining the groups.
Crossover Design
A trial structure in which participants receive multiple interventions in sequence, separated by a washout period, allowing each participant to serve as their own control.
Adverse Event
Any unfavorable or unintended sign, symptom, or condition occurring during a trial, whether or not it’s determined to be related to the intervention being studied.
CONSORT Guidelines
A widely adopted reporting standard (Consolidated Standards of Reporting Trials) that specifies how trial methods, participant flow, and results should be documented to promote transparency and reproducibility.
Ethical Considerations in RCTs
Informed Consent
Participants must be given a clear explanation of the trial’s purpose, procedures, risks, and benefits, and must voluntarily agree to take part before enrollment. Consent must also cover the possibility of being assigned to a control or placebo group rather than the active treatment.
Equipoise
A trial is only considered ethical if there’s genuine uncertainty within the medical or scientific community about which treatment, if any, is more effective. If strong evidence already favors one option, withholding it from a control group becomes difficult to justify.
Right to Withdraw
Participants must be free to leave a trial at any point, for any reason, without penalty or effect on their ongoing care. This right must be communicated clearly at the outset and respected throughout.
Minimizing Harm
Researchers are obligated to design trials that minimize risk to participants, monitor for adverse events throughout the study, and stop the trial early if evidence of serious harm emerges.
Use of Placebo Controls
Withholding treatment via a placebo is ethically acceptable only when no proven effective treatment already exists, or when withholding treatment poses no serious risk to participants’ health.
Vulnerable Populations
Extra safeguards are required when trials involve groups with limited capacity to give full informed consent or an increased risk of coercion, such as children, prisoners, or individuals with cognitive impairments.
Data Monitoring and Early Stopping
Many trials use an independent Data and Safety Monitoring Board (DSMB) to review interim results and recommend stopping the trial early if the intervention proves clearly beneficial, clearly harmful, or unlikely to show a meaningful effect.
Institutional Review Board (IRB) Approval
Before a trial begins, it must be reviewed and approved by an independent ethics committee or Institutional Review Board, which evaluates the study design for compliance with ethical standards and participant protections.
Transparency and Reporting
Ethical conduct extends beyond the trial itself to how results are reported. Trials are increasingly required to be preregistered, and researchers are expected to publish results regardless of whether they support or contradict the hypothesis, to avoid selective reporting bias.
How to Interpret Results of an RCT
Check the p-value, but Don’t Stop There
A p-value below the chosen significance threshold (commonly ) indicates the result is unlikely to have occurred by chance alone, assuming the null hypothesis is true. However, a low p-value doesn’t indicate how large or meaningful the effect is, only that it’s statistically detectable.
Look at the Effect Size
Effect size quantifies the actual magnitude of difference between groups, such as a mean difference, risk ratio, or odds ratio. A statistically significant result with a tiny effect size may have limited real-world relevance, while a large effect size strengthens the case for practical importance.
Examine the Confidence Interval
A 95% confidence interval gives a range of plausible values for the true effect. A narrow interval suggests a more precise estimate, while a wide one signals greater uncertainty, often due to a smaller sample size. If the interval crosses the point of no effect (such as zero for a mean difference or one for a risk ratio), the result may not be statistically significant.
Consider Statistical vs Practical Significance
A result can be statistically significant without being practically meaningful, particularly in large trials where even trivial differences can reach significance. Conversely, a promising but non-significant result in a small trial may still warrant further investigation with a larger sample.
Assess Internal Validity
Review how well the trial controlled for bias: was randomization properly implemented, was blinding used, and was attrition low and balanced between groups? Weaknesses in any of these areas can undermine confidence in the results, regardless of the p-value.
Assess External Validity
Consider whether the trial’s participants, setting, and conditions resemble the population and context you’re interested in. A drug tested only in healthy young adults, for example, may not generalize well to older patients with multiple health conditions.
Look for Subgroup and Sensitivity Analyses
Check whether the reported effect held consistently across subgroups (such as age or disease severity) and whether results remained stable under different analytical approaches, since inconsistent findings across subgroups can indicate the overall result is less reliable than it first appears.
Read Beyond the Abstract
Abstracts can oversimplify or overstate findings. Reviewing the full methods and results sections, including any limitations the authors acknowledge, gives a more complete and accurate picture of what the trial actually shows.
FAQs
What is the gold standard for randomized control trials?
What are the 5 types of clinical trials?
Prevention trials
Diagnostic trials
Screening trials
Quality of life (supportive care) trials
What are the 4 types of studies?
Cohort studies
Case-control studies
Cross-sectional studies